E log of 32 year old male
This is an a online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
A 32 year old male who is a village revenue assistant by occupation came to opd with c/o
Fever since 10 days
Productive cough since 5 days
HOPI:
Patient was apparently asymptomatic 10 days ago then he developed fever which is low grade , intermittent type, Mainly during night time and relived temporarily with medication , associated with chills and rigors.
C/o productive cough with mucoid sputum, intermittent type, which is mainly during night time.
-Generalised weakness present
-Not associated with burning micturition ,cold,rash ,body pains ,vomitings,loose stools
-Associated with sob on doing ordinary activity( grade 2 mmrc) since 5 days , relieves on taking rest
Past history:
Not a k/c/o DM,HTN ,CVA,CAD ,ASTHMA
Patient had a trauma history 5 years back his leg was injured totally, bandage applied for it
He is know case of HIV (diagnosed 1 year ago )and he is on medication
Personal history :
Diet-mixed
Appetite-normal
Sleep-adequate
B and bladder movements-normal
Addictions-toddy -12 years back ,occasionally
Daily routine -
The patient is a village revenue assistant by occupation.He wakes up by 7 am freshens up and takes his breakfast at 8:00am and goes to his work,Then he takes lunch break at 1pm and goes back to work ,he takes dinner by 8 pm and sits with his children for some time the goes to sleep at 9pm.
His daily activities are disturbed. Due to his symptoms
GENERAL EXAMINATION:
-No palor
-No Icterus
-No cyanosis
-No lymphadenopathy
-No edema
-No clubbing of fingers


Temperature:
Febrile - 99.9°F
Pulse: 82 beats per minute
Respiratory rate: —16 cycles per minute
Blood pressure: 130/90 mm of Hg
SYSTEMIC EXAMINATION:
Cardiovascular system:
No thrills
No murumurs
Cardiac sounds: S1, S2 present
Respiratory system:
Bilateral airway entry present ,crepts heard in IAA ,left ISA ,Right IAA
Abdomen:
shape scaphoid
umbilicus central , inverted
no increase in local temp,no tenderness
No spleenomegaly
No hepatomegaly
BS+
Investigations:








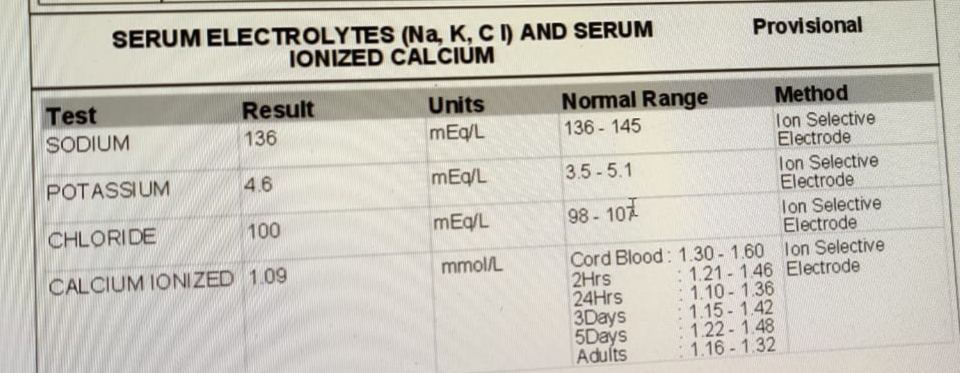

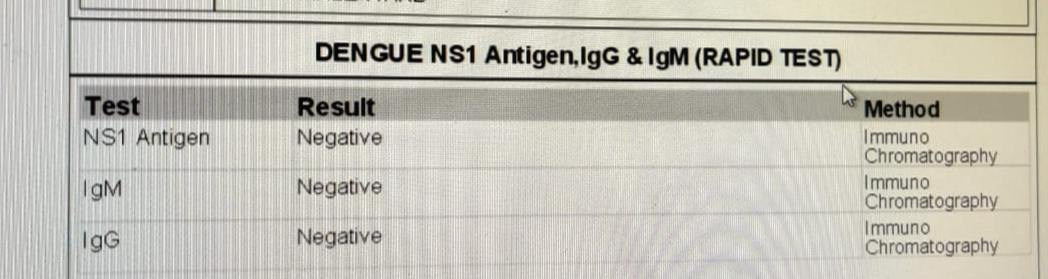

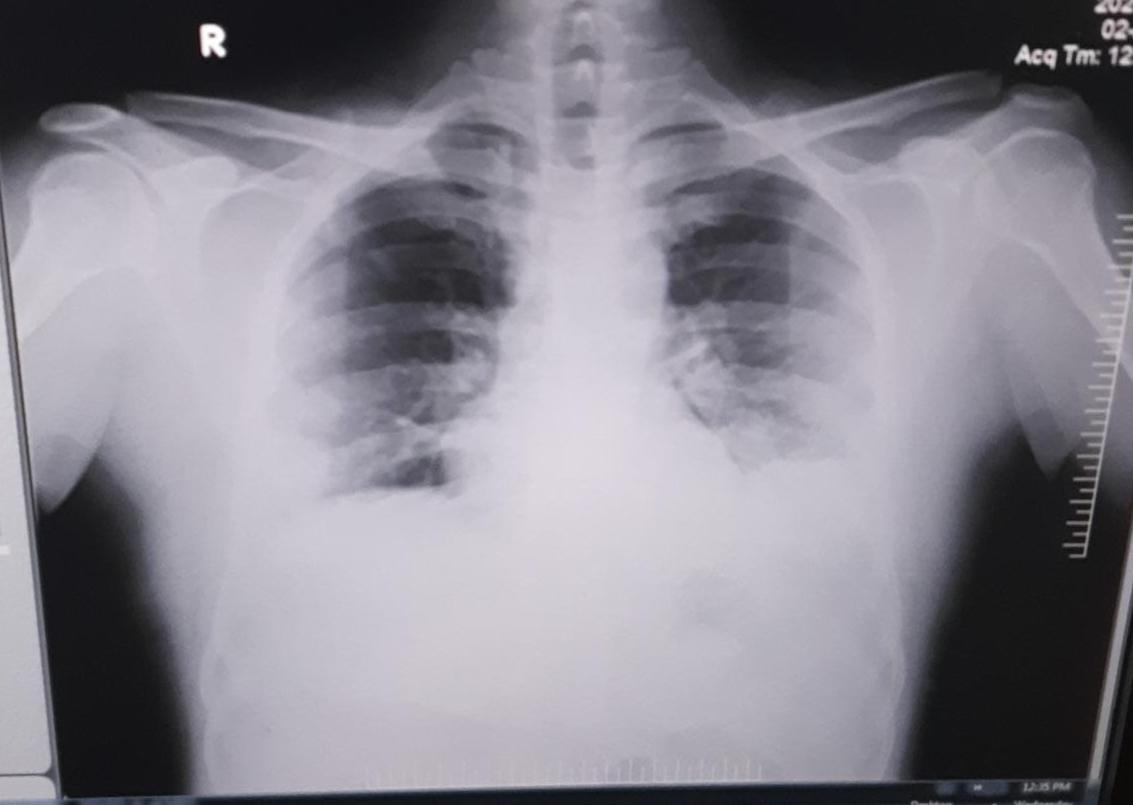

Diagnosis:
Pyrexia under evaluation
?pulmonary Tb
? community acquired pneumonia
.jpeg)

Comments
Post a Comment